Indian Health Service: Actions Needed to Improve Oversight of Quality of Care
Fast Facts
American Indians and Alaska Natives die at higher rates than other Americans from preventable causes—such as diabetes and influenza.
The Indian Health Service is charged with providing health care to these populations, but we found it had limited, inconsistent oversight over the quality of care at its facilities. Among other things, a lack of agency-wide performance standards and significant leadership turnover affected its oversight of quality.
We recommended that IHS develop agency-wide standards for quality care, monitor facility performance in meeting these standards, and develop succession plans for the replacement of key personnel.
Health Care Responsibilities of Indian Health Service Headquarters, Area Offices, and Federally Operated Facilities
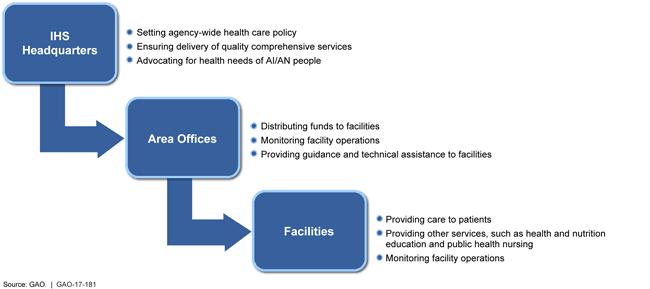
Hierarchy showing policy set by HQ, funds distributed by area offices and facilities providing care.
Highlights
What GAO Found
The Indian Health Service's (IHS) oversight of the quality of care provided in its federally operated facilities has been limited and inconsistent. While some oversight functions are performed at the headquarters level, the agency has delegated primary responsibility for the oversight of care to nine area offices. Area officials stated that the oversight they provide has included, for example, holding periodic meetings with facility staff, reviewing available quality performance data and reviewing adverse events. However, GAO found that this oversight was limited and inconsistent across IHS facilities, due in part to a lack of agency-wide quality of care standards. Specifically, GAO found:
variation in the frequency of governing board meetings and the extent to which quality was a standing agenda item at these meetings;
limited and inconsistent reporting of quality data across IHS areas and facilities; and
inconsistent reporting of adverse events at federally operated facilities.
These inconsistencies are also exacerbated by significant turnover in area leadership. Officials from four of the nine area offices in our review reported that they each had at least three area directors in the past five years. According to IHS officials, the agency has not defined contingency or succession plans for the replacement of key personnel, including area directors. IHS's lack of agency-wide quality of care standards and lack of contingency and succession plans for key personnel are inconsistent with federal internal control standards. These standards suggest that agencies should establish and review performance standards and then monitor data to assess the quality of performance over time, and define contingency and succession plans for the replacement of key personnel to help IHS continue achieving its objectives. As a result, IHS officials cannot ensure that facilities are providing quality health care.
Recognizing the challenges it faces with overseeing and providing quality health care in its facilities, IHS finalized the development of a quality framework in November 2016 that outlines, at a high level, IHS's plan to develop, implement, and sustain a quality program intended to improve patient experience and ensure the delivery of reliably high quality health care. For example, the framework directs IHS to develop a quality office that will be responsible for identifying resource needs, structures, processes, and supports for an effective and sustainable quality assessment and performance improvement system. More specifically, the framework directs IHS to develop a process for monitoring select performance measures, such as measures of clinical care, patient access, and financial performance, for periodic review by leadership. The framework also explains that IHS will enhance its current patient safety reporting systems to encourage consistent use by staff. If effectively implemented, the quality framework could address the limited and inconsistent oversight of the quality of care provided in federally operated IHS facilities. As of November 2016, IHS officials stated that the agency has not yet selected quality performance measures but has plans to do so.
Why GAO Did This Study
IHS is charged with providing health care to American Indian/Alaska Native (AI/AN) people who are members or descendants of 567 tribes. AI/AN people born today have a life expectancy that is 4.4 years lower than all races in the United States, and they continue to die at higher rates than other Americans from preventable causes. Concerns about the quality of care provided to AI/ANs in IHS facilities have been identified recently by federal officials and tribal members. GAO was asked to review how IHS oversees the quality of care provided in its facilities.
This report examines IHS's oversight of the quality of care provided in its federally operated facilities. GAO reviewed policies and guidance related to quality of care in federally operated facilities and interviewed IHS officials at the headquarters level and all nine area offices with federally operated facilities. GAO also examined documents from governance meetings between area office and facility staff.
Recommendations
GAO recommends that the Secretary of the Department of Health and Human Services direct the Director of IHS to (1) as it implements its quality framework, ensure that agency-wide standards for the quality of care provided in its federally operated facilities are developed, that facility performance in meeting these standards is monitored over time, and that enhancements are made to its adverse event reporting system, and (2) develop contingency and succession plans for the replacement of key personnel.
HHS concurred with GAO's recommendations.
Recommendations for Executive Action
| Agency Affected | Recommendation | Status |
|---|---|---|
| Department of Health and Human Services |
Priority Rec.
To help ensure that quality care is provided to AI/AN people, as part of the implementation of its quality framework, the Secretary of HHS should direct the Director of IHS to ensure that agency-wide standards for the quality of care provided in its federally operated facilities are developed, that facility performance in meeting these standards is systematically monitored over time, and that enhancements are made to its adverse event reporting system. |
HHS concurred with this recommendation and cited steps that have been taken to improve the quality of care in IHS's federally-operated facilities, including establishing an IHS Office of Quality, and developing a dashboard of standards for quality of care. In addition, in August 2020, IHS completed implementation of a new adverse event reporting system. The IHS Safety Tracking and Response (I-STAR) system is a portal for reporting "good catches" (near misses), along with patient/visitor, medication, and occupation safety events. IHS officials stated they will monitor I-STAR utilization through regular system audits, and that adverse event monitoring occurs at facilities through reports to Governing Boards with additional oversight by IHS's Quality Assurance Risk Management Committee.
|
| Department of Health and Human Services | To help ensure that quality care is provided to AI/AN people, as part of the implementation of its quality framework, the Secretary of HHS should direct the Director of IHS to develop contingency and succession plans for the replacement of key personnel, including area directors. |
In December 2016, the IHS Principal Deputy Director issued a directive for all HQ and Area Offices to develop succession and contingency plans to identify potential leaders or senior managers to fill critical positions in the short- or the long-term, and identify individuals available immediately for unexpected absences or departures. The IHS Office of Human Resources (OHR) issued guidance, instructions, and a template for identifying key leadership positions in the HQ Offices, Area Offices, and Service Units. All HQ and Area Offices submitted a plan to the IHS OHR. On August 8, 2017, all HQ and Area Office Directors received a request from the Director, OHR to update their respective Office/Area plans. In that message, HQ and Area Office Directors also received the original guidance that was sent out in December 2016 that included the requirement to identify staff and development needs to prepare for future leadership opportunities and to plan for any immediate needs.
|