Medicare: Information on Medicare-Dependent Hospitals
Fast Facts
Medicare pays hospitals set amounts based on the diagnoses of the Medicare patients they serve. Small, rural hospitals that meet certain eligibility criteria can qualify for additional payments.
If those hospitals serve a high proportion of Medicare patients, they can apply for the additional payments under the Medicare-dependent hospital program. We found that between 2011 and 2017:
The number of Medicare-dependent hospitals decreased by about 28% because, for example, they became ineligible for the program, merged with other hospitals, or closed.
The typical Medicare-dependent hospital saw profits decrease by almost 2 percentage points.
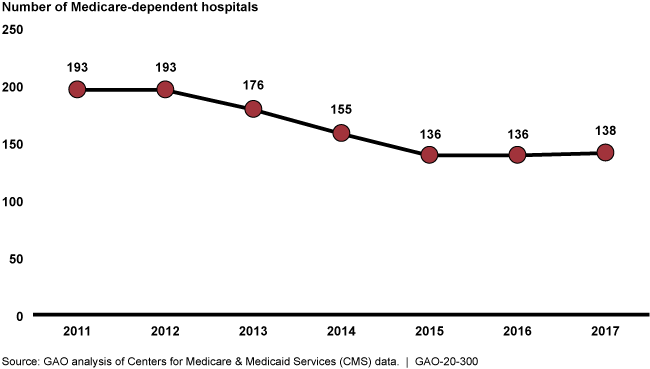
Line graph showing 193 in 2011; 193 in 2012; 176 in 2013; 155 in 2014; 136 in 2015; 136 in 2016; and 138 in 2017
Highlights
What GAO Found
The Centers for Medicare & Medicaid Services (CMS) operates the Medicare-dependent Hospital (MDH) program, which assists hospitals that have 60 percent or more of inpatient days or discharges from Medicare patients, 100 or fewer beds, and that are generally located in a rural area. MDHs receive an additional payment if their historic costs in one of three base years adjusted for inflation, among other things, are higher than what the hospital would have otherwise received under the inpatient prospective payment system (IPPS). In contrast, if the IPPS amount was higher than historic costs, the MDH would receive no additional payment. In fiscal year 2018, CMS paid approximately $119 million in additional payments to MDHs.
From fiscal years 2011 through 2017, the number of MDHs declined by around 28 percent. (See figure.) In addition, the number of MDHs that received an additional payment declined by around 15 percent.
Figure: Number of Medicare-Dependent Hospitals, Fiscal Years 2011 through 2017
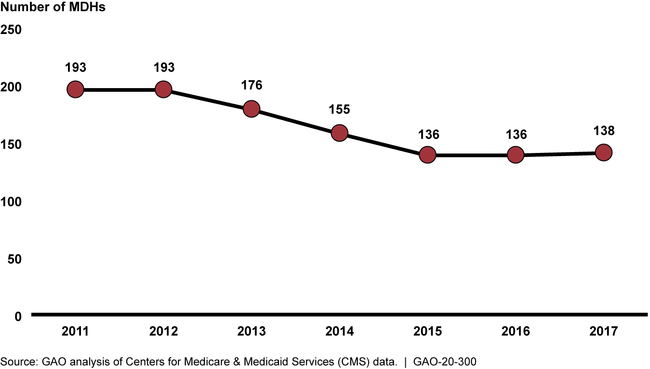
Over this period of time, MDHs also experienced a 13 percent decrease in the share of their Medicare revenue that came from inpatient services. In addition, there was a decline in the share of total MDH revenue that was attributed to Medicare patients, and a decline in Medicare profit margins by about 6 percentage points.
Why GAO Did This Study
The MDH program was enacted in 1989, providing a financial benefit to some small, rural hospitals with high shares of Medicare patients. The original MDH program was established through statute for 3 years, and Congress has extended it on several occasions. The Bipartisan Budget Act of 2018 included a provision to extend the MDH program through 2022, as well as a provision for GAO to review the MDH program.
This report describes, among other things, the changes that occurred in the number of MDHs and selected metrics over time. GAO analyzed data submitted to CMS by hospitals from fiscal years 2011 through 2017—the most recent year for which consistent data were available at the time of GAO's analysis—among other CMS data. GAO also reviewed CMS regulations and other agency documents.
The Department of Health and Human Services provided technical comments on a draft of this report, which GAO incorporated as appropriate.
For more information, contact Jessica Farb at (202) 512-7114 or farbj@gao.gov.