Hospital Value-Based Purchasing: Initial Results Show Modest Effects on Medicare Payments and No Apparent Change in Quality-of-Care Trends
Highlights
What GAO Found
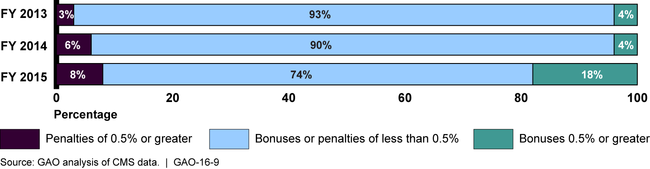
The bonuses and penalties received by most of the approximately 3,000 hospitals eligible for the Hospital Value-based Purchasing (HVBP) program amounted to less than 0.5 percent of applicable Medicare payments each year. GAO found that safety net hospitals, which provide a significant amount of care to the poor, consistently had lower median payment adjustments—that is, smaller bonuses or larger penalties—than hospitals overall in the program's first three years. However, this gap narrowed over time. In contrast, small urban hospitals had higher median payment adjustments each year than hospitals overall, and small rural hospitals' median payment adjustments were similar to hospitals overall in the first two years and higher in the most recent year.
Figure: Distribution of Hospital Value-based Purchasing Bonuses and Penalties Greater Than or Less Than 0.5 Percent, Fiscal Years 2013 through 2015
GAO's analysis found no apparent shift in existing trends in hospitals' performance on the quality measures included in the HVBP program during the program's initial years. However, shifts in quality trends could emerge in the future as the HVBP program continues to evolve. For example, new quality measures will be added, and the weight placed on clinical process measures—on which hospitals had little room for improvement—will be substantially reduced. For many quality measures not included in the HVBP program, GAO also found that trends in hospitals' performance remained unchanged in the period GAO reviewed, but there were exceptions in the case of three measures that are part of a separate incentive program targeting hospital readmissions. This program focuses exclusively on readmissions and imposes only penalties. The timing of changes in readmission trends provides some indication that the use of financial incentives in quality improvement programs may, under certain circumstances, promote enhanced quality of care. However, understanding the extent of that impact depends on the results of future research.
Officials from selected hospitals GAO interviewed reported that the HVBP program generally reinforced ongoing quality improvement efforts, but did not lead to major changes in focus. In addition, hospital officials cited a variety of factors that affected their capacity to improve quality. For example, officials from most hospitals GAO contacted reported challenges related to using information technology (IT) systems—including electronic health records—to make quality improvements. In contrast, other hospital officials said their IT systems aided their quality performance efforts, such as by helping to collect clinical data needed to track progress on quality measures. Hospital officials described such factors as affecting their hospital's quality improvement efforts as a whole, rather than being specifically linked to implementation of the HVBP program.
Why GAO Did This Study
The HVBP program, which the Centers for Medicare & Medicaid Services (CMS) administers, annually evaluates individual hospital performance on a designated set of quality measures related to inpatient hospital services and, based on those results, adjusts Medicare payments to hospitals in the form of bonuses and penalties. The HVBP program was enacted in 2010 as part of the Patient Protection and Affordable Care Act (PPACA). The first HVBP payment adjustments occurred in fiscal year 2013.
PPACA included a provision for GAO to assess the HVBP program's impact on Medicare quality and expenditures, including the HVBP program's effects on small rural, small urban, and safety net hospitals. This report evaluates the initial effects of the HVBP program on: (1) Medicare payments to hospitals, (2) quality of care provided by hospitals, and (3) selected hospitals' quality improvement efforts. To determine these initial effects of the HVBP program, GAO analyzed CMS data on bonuses and penalties given to hospitals in fiscal years 2013 through 2015 as well as data on hospital quality measures collected by CMS from 2005 through 2014, the most recent year available. GAO also interviewed officials with eight hospitals that participated in the HVBP program. Hospitals were selected to include safety net, small urban, and small rural hospitals, as well as those that were not part of any of these subgroups.
The Department of Health and Human Services, which includes CMS, reviewed a draft of this report and provided technical comments, which GAO incorporated as appropriate.
For more information, contact Linda Kohn at (202) 512-7114 or kohnl@gao.gov.