VA Health Care: Actions Needed to Assess Decrease in Root Cause Analyses of Adverse Events
Highlights
What GAO Found
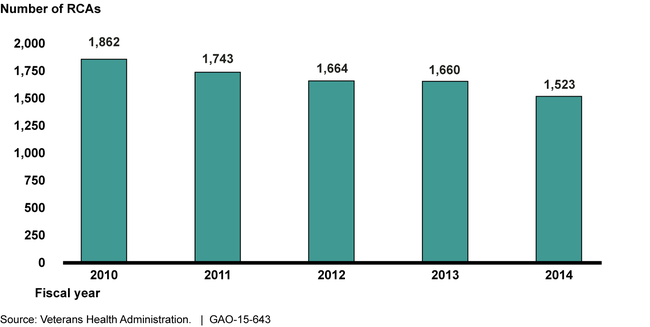
To address adverse events, Department of Veterans Affairs (VA) medical centers (VAMC) completed 18 percent fewer root cause analyses (RCA) in fiscal year 2014 compared to fiscal year 2010, and the Veterans Health Administration (VHA) has not analyzed the reasons for the decrease. VHA's National Center for Patient Safety (NCPS) officials told GAO they were aware of the decrease, but were not certain why the number of completed RCAs had decreased over time, especially in light of a 7 percent increase in reports of adverse events over the same time period. NCPS officials suggested several potential factors that could contribute to the decrease, including VAMCs' use of processes other than RCAs to address adverse events. However, NCPS is unaware of how many VAMCs use these other processes or their results. VHA's lack of analysis is inconsistent with federal internal control standards which state that agencies should compare data to analyze relationships and take appropriate actions. Because NCPS has not conducted an analysis of the relationship between the decrease in RCAs and possible contributing factors, it is unclear whether the decrease indicates a negative trend in patient safety at VAMCs or a positive one. In addition, without understanding the extent to which VAMCs use alternative processes and their results, NCPS has limited awareness of what VAMCs are doing to address the root causes of adverse events.
RCAs Completed at VAMCs, Fiscal Years 2010 through 2014
NCPS oversees the RCA process by monitoring VAMC compliance, and develops system-wide patient safety initiatives informed by RCA data. NCPS monitors each VAMC's compliance with requirements by reviewing RCA database information and conducting site visits. NCPS uses RCA information to inform system-wide patient safety initiatives, such as Patient Safety Alerts and Advisories—urgent notifications sent to VAMCs that describe a safety issue and include instructions and due dates for implementing actions to prevent recurrence.
Why GAO Did This Study
Adverse events are incidents that pose a risk of injury to a patient as the result of a medical intervention or the lack of an appropriate intervention. VAMCs use the RCA process to identify and evaluate systems or processes that caused an adverse event, recommend changes to prevent the event's recurrence, and determine whether implemented changes were effective.
GAO was asked to review VA's processes and procedures for responding to adverse events. In this report, GAO examined (1) the extent to which VAMCs used the RCA process to respond to adverse events and (2) how VHA oversees the RCA process and uses information from the process to make system-wide improvements. To conduct this work, GAO reviewed VHA policy and guidance documents, analyzed VHA data on RCAs completed from fiscal years 2010 through 2014, and interviewed officials from NCPS—the VHA office responsible for monitoring RCA data. GAO also analyzed local RCA data and interviewed officials from four VAMCs selected to provide variation in factors such as complexity and location.
Recommendations
GAO recommends that VA (1) analyze the declining number of completed RCAs, including identifying the contributing factors and taking appropriate actions, and (2) determine the extent to which VAMCs are using alternative processes to address adverse events, and collect information on their results. VA concurred with GAO's recommendations.
Recommendations for Executive Action
| Agency Affected | Recommendation | Status |
|---|---|---|
| Department of Veterans Affairs | To ensure that appropriate steps are being taken to address the root causes of adverse events within VHA, the Secretary of Veterans Affairs should direct the Under Secretary for Health to conduct an analysis of the declining number of completed RCAs within the VA health care system, including identifying contributing factors, and take appropriate actions to address them. |
In September 2016, Department of Veterans Affairs (VA) National Center for Patient Safety (NCPS) officials stated that they would charter an interdisciplinary team of internal and external VHA members by October 30, 2016 to reevaluate and/or supplement the root causes/contributing factors delineated in their previous actions. We noted in our report that NCPS knew about possible contributing factors, but without an analysis it was unclear whether the difference between the number of incident reports (a 7 percent increase from fiscal year 2010 through fiscal year 2014) and total completed RCAs (an 18 percent decrease from fiscal year 2010 through fiscal year 2014) was a cause for concern. In February 2017, the interdisciplinary team issued a report that used root cause analysis (RCA) methods to examine the factors and organizational impediments that prevented VHA from addressing the problems that led to a decrease in RCAs. The report identified both proximate causes (high turnover of patient safety managers at VA medical centers) and distal causes (a deterioration of the culture of safety at VA medical centers) for the decrease in RCAs. The report also included recommendations for further actions VHA can take to address the proximate and distal causes. NCPS officials told us that modifications made in FY2015 and FY2016 to a VA medical center NCPS recognition program have already addressed some of the report's proximate and distal causes and the Assistant Deputy Under Secretary for Quality, Safety, and Value is responsible for addressing other causes as warranted. We believe VHA's actions have satisfied the intent of our recommendation and we consider this recommendation implemented.
|
| Department of Veterans Affairs | To ensure that appropriate steps are being taken to address the root causes of adverse events within VHA, the Secretary of Veterans Affairs should direct the Under Secretary for Health to determine the extent to which VAMCs are using alternative processes to address the root causes of adverse events when an RCA is not required, and collect information from VAMCs on the number and results of those alternative processes. |
In September 2015, the Department of Veterans Affairs National Center for Patient Safety (NCPS) developed and fielded a survey to all medical centers to assess what degree they were utilizing alternative processes to address root causes of adverse events when a root cause analysis is not required. NCPS was able to obtain data from 86 percent of medical centers that demonstrated the types of alternative processes used and how medical centers were using them. As a result, we are closing this recommendation as implemented.
|